



文章来源:医脉通
在芝加哥当地时间5月30日上午的ASCO临床科学论坛上,马德里Universitario 12 de Octubre医院的Luis Paz-Ares教授带来了关于Nivolumab延长非鳞状非小细胞肺癌患者生存的重要研究(摘要LBA109)。医脉通对此进行了报道。
这项III期随机试验结果显示PD-1免疫疗法对于非鳞状非小细胞肺癌有效。对于以铂类为基础的化疗失败的晚期患者,使用nivolumab治疗比多西他赛化疗,患者平均存活时间长3个月。
该研究第一作者,来自西班牙马德里Universitario 12 de Octubre医院医学系教授Luis Paz-Ares表示,“这是第一个证明免疫治疗对非鳞状非小细胞肺癌、尤其是PD-L1阳性的肺癌有效的三期临床研究。 nivolumab除了比作为标准二线治疗的多西他赛化疗效果更好外,其使用更加容易。”
肺癌是全世界最常见的肿瘤,2012年就有超过180万新发肺癌病例。在美国,肺癌是癌症死亡的首要原因。而非小细胞肺癌是最常见的肺癌类型,占到了肺癌85%的比例,这其中2/3以上为非鳞细胞癌类型。
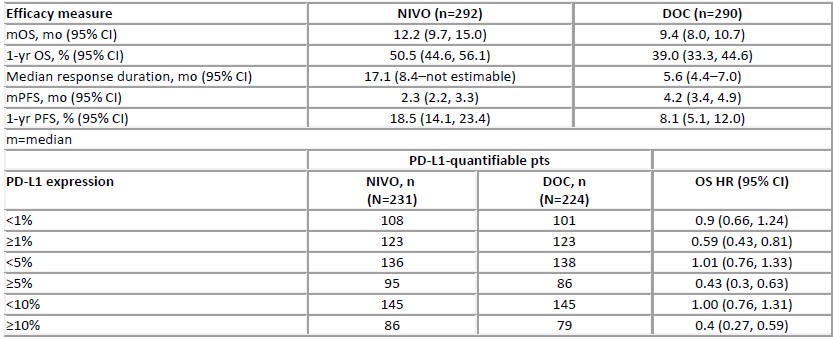
该研究纳入了582例晚期非鳞状非小细胞肺癌患者,将其随机分配到nivolumab治疗组或多西他赛治疗组。结果显示nivolumab组的缓解率高于多西他赛组(19.2% vs. 12.4%),且缓解显著延长(平均17.1月 vs. 5.6 月)。
nivolumab组的中位生存期为12.2月,多西他赛组中位生存期为9.4月。值得注意的是,nivolumab组中具有高水平PD-L1 (≥1% 细胞)的患者中位生存期超过了17个月,而多西他赛组中这类患者中位生存期为9个月。
总体来说,患者对Nivolumab耐受性好,仅有十分之一的患者出现严重副反应,而多西他赛组中超过半数的患者出现严重副反应。多西他赛组中出现1例治疗相关死亡,而nivolumab组无死亡报道。分别有4.9%和14.9%的患者因药物毒性反应停止了nivolumab和多西他赛的治疗。停止治疗的患者有将近一半随后接受了全身治疗。
研究指出具有高水平PD-L1的患者使用nivolumab治疗的获益最大。总之,接受nivolumab治疗比多西他赛治疗死亡风险降低27%。其中高表达PD-L1的亚组患者使用nivolumab治疗死亡风险下降41- 60%,但这一获益在低水平PD-L1或不可检测的患者中并未观察到。
今年早些时候,美国FDA批准nivolumab作为晚期肺鳞癌的二线治疗用药。但在欧洲nivolumab仍未被批准使用。Paz-Ares博士指出nivolumab有可能成为既往接受过治疗的非小细胞肺癌患者的新的标准治疗方法。
摘要原文
Background: Options for advanced non-SQ NSCLC patients (pts) who progress after platinum-based doublet chemotherapy (PT-DC) are limited, with minimal improvement in overall survival (OS). We report results from a randomized, global phase III study of NIVO, a fully human IgG4 programmed death-1 (PD-1) immune checkpoint inhibitor antibody, vs DOC in pts with advanced non-SQ NSCLC after failure of PT-DC and tyrosine kinase inhibitor, if eligible.
Methods: Pts were randomized to NIVO 3 mg/kg Q2W (n=292) or DOC 75 mg/m2 Q3W (n=290) until progression or discontinuation due to toxicity/other reasons. Primary objective was OS; secondary objectives were investigator-assessed objective response rate (ORR; per RECIST v1.1), progression-free survival (PFS), efficacy by PD-L1 expression, quality of life, and safety.
Results: NIVO demonstrated superior OS (HR=0.73; 96% CI: 0.59, 0.89; P=0.00155) and improved ORR (19.2% vs 12.4%; P=0.0235). HR for PFS was 0.92 (95% CI: 0.77, 1.11; P=0.393). PD-L1 expression was associated with benefit from NIVO (Table). In PD-L1+pts, NIVO showed improved efficacy across all endpoints at predefined 1%, 5%, and 10% cut-points. Grade 3–5 drug-related AEs occurred in 10.5% (30/287) of NIVO and 53.7% (144/268) of DOC pts. No deaths were related to NIVO vs 1 DOC-related death. After discontinuation, 42.1% of NIVO and 49.7% of DOC pts received subsequent systemic therapy.
Conclusions: NIVO demonstrated superior OS vs DOC in pts with advanced non-SQ NSCLC after failure of PT-DC. The safety profile of NIVO 3 mg/kg Q2W was favorable vs DOC. NIVO demonstrated survival benefit across histologies in two randomized phase III trials.